









This website uses cookies to help improve your user experience




Telemedicine has moved from convenience to infrastructure. Millions of clinical interactions now happen over video: diagnoses delivered, prescriptions discussed, mental health sessions conducted from living rooms and hospital wards alike.
The technology behind that shift carries a legal and ethical obligation that doesn’t shrink because the care is remote. This guide breaks down what HIPAA compliance actually requires from video conferencing platforms, where the risks concentrate, and what it takes to build or choose a solution that holds up under scrutiny.
Key takeaways:
For any organization that handles patient health data, HIPAA is the legal framework that determines how that data must be protected, not a regulatory acronym to file away and forget.
The Health Insurance Portability and Accountability Act sets out what healthcare organizations and their technology partners are required to do. It mandates administrative, physical, and technical safeguards around every stage of how protected health information (PHI) moves, lives, and gets accessed.
When those safeguards fall short, it’s the HHS Office for Civil Rights (OCR) that comes knocking, investigating complaints, auditing compliance programs, and issuing penalties. In telemedicine, where every clinical interaction crosses a network, getting those safeguards right starts with the platform delivering the care.
Real-time video communication is reshaping how care reaches patients, closing gaps that geography, mobility, and overwhelmed schedules have long made difficult to bridge.
However, transmitting clinical conversations and health records over video networks puts protected health information directly in the line of exposure. Under HIPAA’s Privacy and Security Rules, any electronic exchange of personal health data, ePHI, carries strict obligations.
Healthcare providers must maintain its confidentiality, guard its integrity, and secure it against unauthorized access. When the entire encounter happens over a network, that responsibility doesn’t shrink. It sharpens.
HIPAA compliance in this context goes beyond avoiding penalties. It shapes patient willingness to engage honestly during remote consultations, particularly in sensitive specialties like mental health. HIPAA compliant video conferencing for therapists carries additional weight around disclosure and trust.
Organizations that treat compliance as an architectural requirement rather than a post-deployment checklist are better positioned to scale telehealth without accumulating regulatory and reputational risk.
HIPAA prescribes relevant safeguards and controls — administrative, physical, and technical — to protect the flow of health data, while ensuring patients’ privacy and giving them greater control over their health information.
In healthcare, the regulatory environment leaves little room for gaps. Civil penalties now range from $145 to over $2.1 million per violation depending on the degree of negligence, with criminal exposure, like fines up to $250,000 and potential imprisonment, in the most serious cases1. OCR’s 2026 enforcement expansion into risk management signals that regulators want to see organizations actively governing their security posture, not just passing periodic audits.
In telehealth specifically, the risk surface is broad. Unencrypted video sessions, misconfigured access controls, missing Business Associate Agreements with platform vendors, and inadequate audit logging have all been featured in OCR enforcement actions. A breach triggers more than a fine — it initiates an investigation into the organization’s entire compliance program, often exposing systemic gaps that carry their own penalties.
That’s what makes selecting the HIPAA compliant teleconferencing solution more consequential than a typical software decision. A good platform should do more than tick the compliance box. It should actively support the organization’s ability to manage and justify its risk decisions.
Just as in a physical consultation, what happens between a clinician and patient must stay between them. But digital channels introduce a different class of exposure: video and audio streams, session recordings, screen sharing, and file transfers each represent a potential point where PHI can be intercepted, stored insecurely, or accessed without authorization.
What HIPAA requires from telemedicine video conferencing becomes clearer when you look at its core technical and operational components.
HIPAA’s access control requirements follow a straightforward principle: the right people should see only what they need to do their jobs, nothing more. In practice, enforcing that principle across video conferencing requires layering several technical controls.
Unique user identification is the starting point. Every user gets a distinct identifier that follows them across devices, creating an audit trail that makes it possible to verify who accessed what, and when. It’s a critical capability when PHI is in motion during a live session.
Role-based access control (RBAC) takes that further by segmenting users according to their clinical or administrative function. A billing coordinator and an attending physician may both use the same platform, but their access to patient data during or after a session should look nothing alike. RBAC makes that segmentation manageable at scale without requiring manual permission reviews for every user.
Encryption sits at the foundation of all of it. HIPAA classifies encryption as “addressable” rather than required, but that distinction is narrower than it sounds. Organizations must either implement it or document a comparable alternative. In video conferencing, there is no credible alternative. 256-bit AES encryption is the clinical and industry standard, protecting in-session data end-to-end so that intercepted streams remain unreadable to anyone outside the authorized call.
Strong authentication is the backbone of any security strategy. It implies verifying that a person or entity is what they claim to be before granting access to ePHI. Passwords paired with biometric authentication, such as facial recognition or fingerprints, add an extra layer of security to protect HIPAA-compliant video conferencing platforms. Biometric authentication is effective and accurate, keeping patient data accessible only to those cleared to see it.
The safest method of authentication is the one that utilizes biometric information like facial features, irises, fingerprints, voice, or keystroke behavior. Unique and nearly impossible to steal, biometrics deliver accurate identification and strengthen the compliance posture of your telemedicine video conferencing solution2.
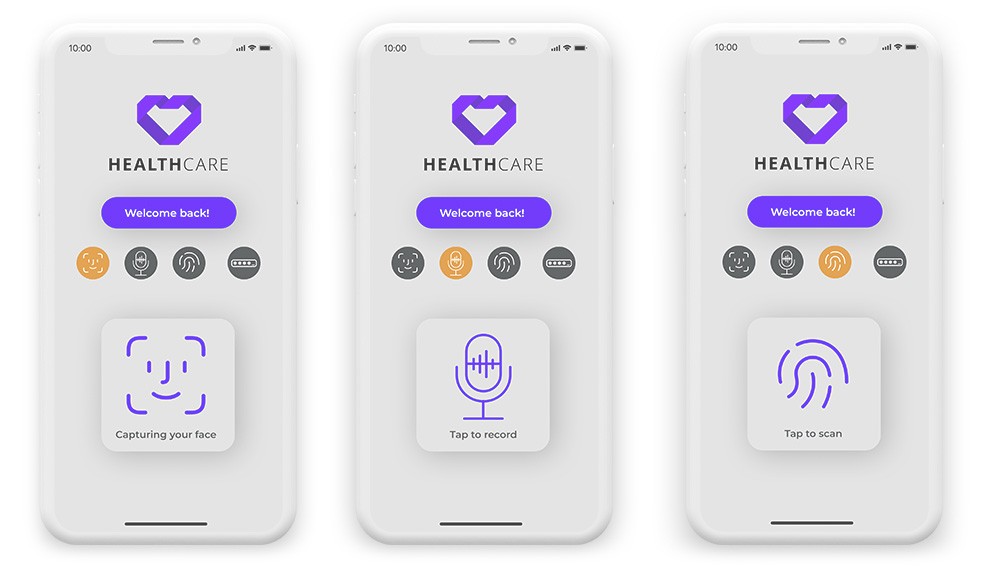

Oxagile’s machine learning and computer vision work powers production-grade authentication — facial recognition, voice biometrics, fingerprint recognition, and keystroke dynamics. These are built to hold up across platforms, devices, and clinical environments where identity verification can’t afford to fail.
If this is part of your telemedicine build, see what we can bring to it.
Every telehealth session is a data exchange in motion: diagnoses, prescriptions, and personal histories passing between patient and clinician through video, audio, screen shares, and file transfers. Unencrypted virtual consultations put that information at direct risk of interception, and data in transit is inherently the most exposed point in that chain. Man-in-the-middle (MITM) attacks exploit exactly this window, inserting an unauthorized party into the communication stream before either participant realizes anything is wrong.
AES-based encryption closes that window, protecting ePHI both at rest and during transmission. Alongside it, Secure Real-Time Transport Protocol (SRTP) handles the live call layer specifically, keeping video and audio streams between browsers encrypted and intact, without the latency that heavier security measures can introduce.
Healthcare is among the costliest sector for data breaches, averaging $7.42 million per incident3. A reminder that the communication infrastructure beneath a telemedicine platform carries clinical liability, not technical complexity alone.
Compromised health data is more than a compliance failure. A modified prescription or altered diagnosis delivered through a tampered telehealth session can directly affect clinical decisions. Under the Security Rule, healthcare providers have to protect ePHI against unauthorized alteration or destruction, apart from unauthorized access.
End-to-end encryption makes ePHI resistant to tampering in transit but doesn’t confirm data arrived exactly as sent. Digital signatures authenticate the source and flag modifications, while checksum verification detects corruption in transmitted data. This way, what the clinician receives matches precisely what was sent.
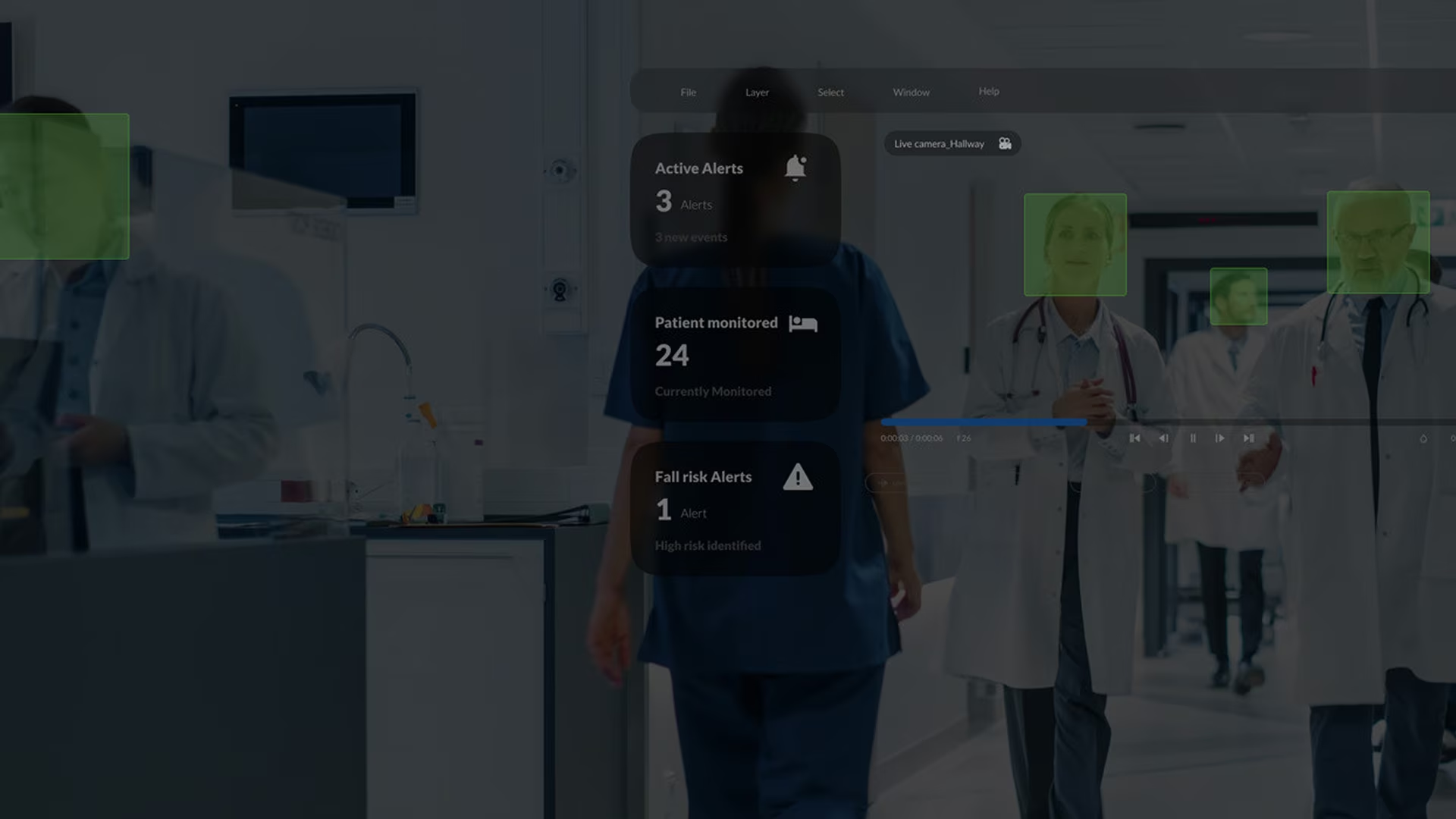
Healthcare is a highly regulated industry, meaning that detailed activity logs and audit trails must be presented for all systems using ePHI. By logging key actions, access threads, modifications, and more, these audit logs are instrumental in detecting security violations and unauthorized access to protected data.
To create a complete audit trail, all details of a video conference session need to be captured, including video, audio, and metadata. Since this granular auditing generates massive amounts of data, make sure your telemedicine solution’s analytic capabilities are adequate to process large volumes of information, identify suspicious patterns, and deliver granular audit reports.
A U.S.-based company delivering hospital-grade video monitoring ran into stability issues as patient volume scaled. Oxagile’s audit identified gaps in connection management and system observability that were undermining performance under clinical load. The engagement covered:
The result: stable video performance at scale and an infrastructure the team could monitor, diagnose, and defend.
Not all video platforms are built for clinical use. The solutions below have established track records in healthcare, sign Business Associate Agreements (BAAs), and implement the technical safeguards HIPAA requires.
The right choice depends on the size of the organization, existing infrastructure, and how deeply video needs to integrate into clinical workflows. Off-the-shelf platforms cover common use cases well. Organizations with more complex workflows or custom requirements often find that purpose-built healthcare solutions deliver better long-term fit.
Telemedicine’s clinical and economic case is well established, but the privacy obligations that come with it are non-negotiable. Patients sharing sensitive health information over a video call deserve the highest level of confidentiality, and HIPAA video conferencing sets the floor for what that requires.
Getting this right is an architectural decision that shapes every layer of the platform, from how data moves to who can access it and when. It’s the starting point for any telemedicine HIPAA compliant video conferencing software.
We build telemedicine video conferencing solutions engineered for clinical reality: low latency, high scalability, and security that holds up under HIPAA scrutiny. End-to-end encryption, biometric authentication, and enterprise-grade architecture aren’t add-ons, they are the foundation.
1. HHS adjusts 2026 HIPAA, certain ACA and MSP monetary penalties — Mercer
2. Healthcare Digital Authentication Market Size and Companies (2026-2035) — Towards Healthcare
3. Cost of a Data Breach Report 2025 — IBM

Compliance comes down to three layers: technical safeguards (end-to-end encryption, access controls, audit logging), administrative alignment with the organization’s broader HIPAA policies, and a signed Business Associate Agreement (BAA) with the vendor. That last point is often underestimated. When evaluating the best HIPAA compliant video conferencing options, the BAA is the most reliable first filter. A platform with strong security features that won’t sign a BAA is not compliant for clinical use.
The privacy obligations are the same, but the technical requirements differ. Traditional phone calls occupy a regulatory gray area that OCR has historically treated with some flexibility. Video conferencing transmits richer data, like shared screens, recorded sessions, metadata, and falls squarely under the Security Rule’s full technical safeguard requirements: encryption, access controls, and audit trails. Session recording adds further obligations around retention, access, and disposal of stored PHI.
The compliance burden falls on the provider, but both connections matter in practice. HIPAA doesn’t regulate the patient’s network, yet an intercepted session is still a breach regardless of where the vulnerability originated.
Providers should give patients straightforward pre-appointment guidance: use a private Wi-Fi network, join from a private space, and keep devices updated. It doesn’t shift legal liability, but it meaningfully reduces the risk of an incident that’s difficult to explain to OCR.

