
By analyzing operational metrics, AI identifies bottlenecks and allocates resources dynamically. Hospitals and clinics can reduce wait times, balance staff workloads, and adjust schedules in real time, making day-to-day operations more efficient.

AI instruments examine patient data and operational metrics to support clinical decisions and care coordination. When used effectively, they reveal patterns, lighten triage, and help clinical teams cut costs and make faster, more informed decisions.
 Optimize
Optimize By analyzing operational metrics, AI identifies bottlenecks and allocates resources dynamically. Hospitals and clinics can reduce wait times, balance staff workloads, and adjust schedules in real time, making day-to-day operations more efficient.
 Personalize
Personalize Medical history, genetics, and real-time patient data can form the foundation for individualized treatment plans. Clinicians can prioritize interventions, anticipate patient needs, and improve engagement, so care methods align with each patient’s unique condition.
 Automate
Automate Routine documentation, billing, and diagnostic flagging are handled automatically, freeing clinicians to focus on patient care. Automating time-consuming processes cuts errors, accelerates service delivery, and allows staff to dedicate more time to high-value work.



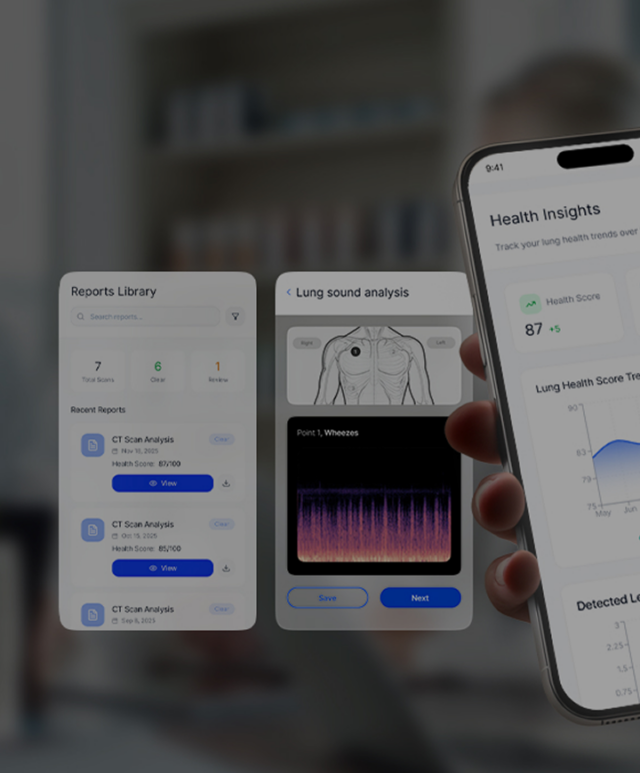
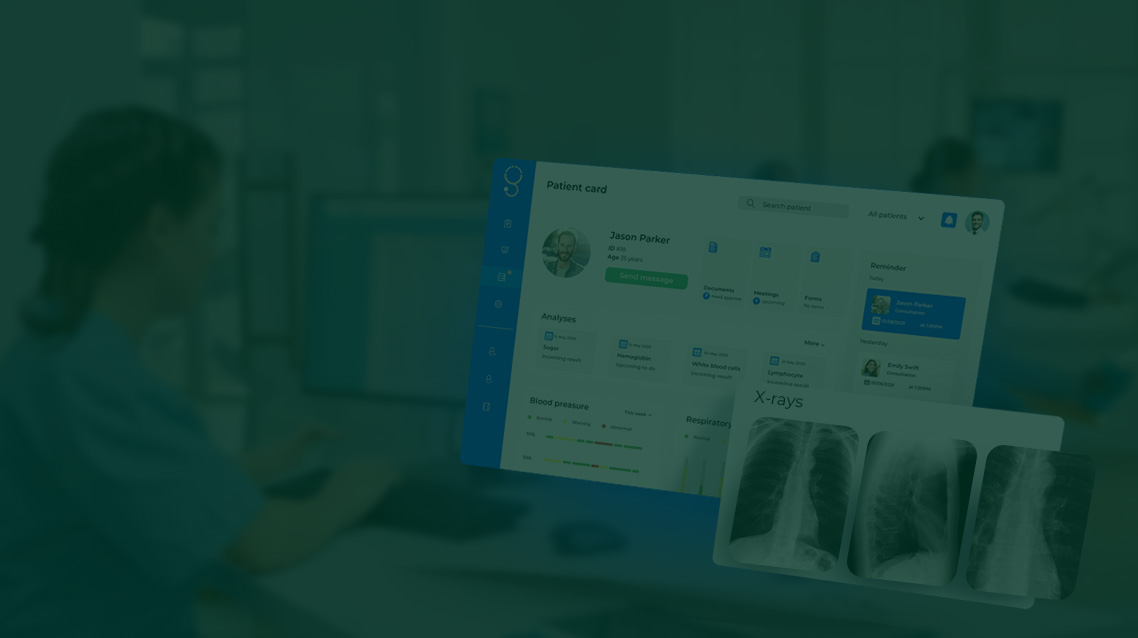
AI systems can detect diseases earlier, plan treatments more accurately, and improve management of patient records, supporting precision and personalized care. It assists clinicians by recommending treatments, flagging potential risks, and analyzing large volumes of patient data to support decision-making.
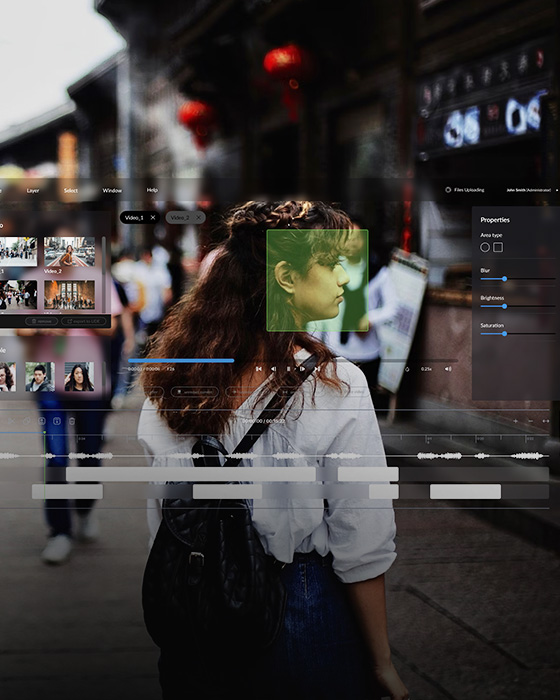
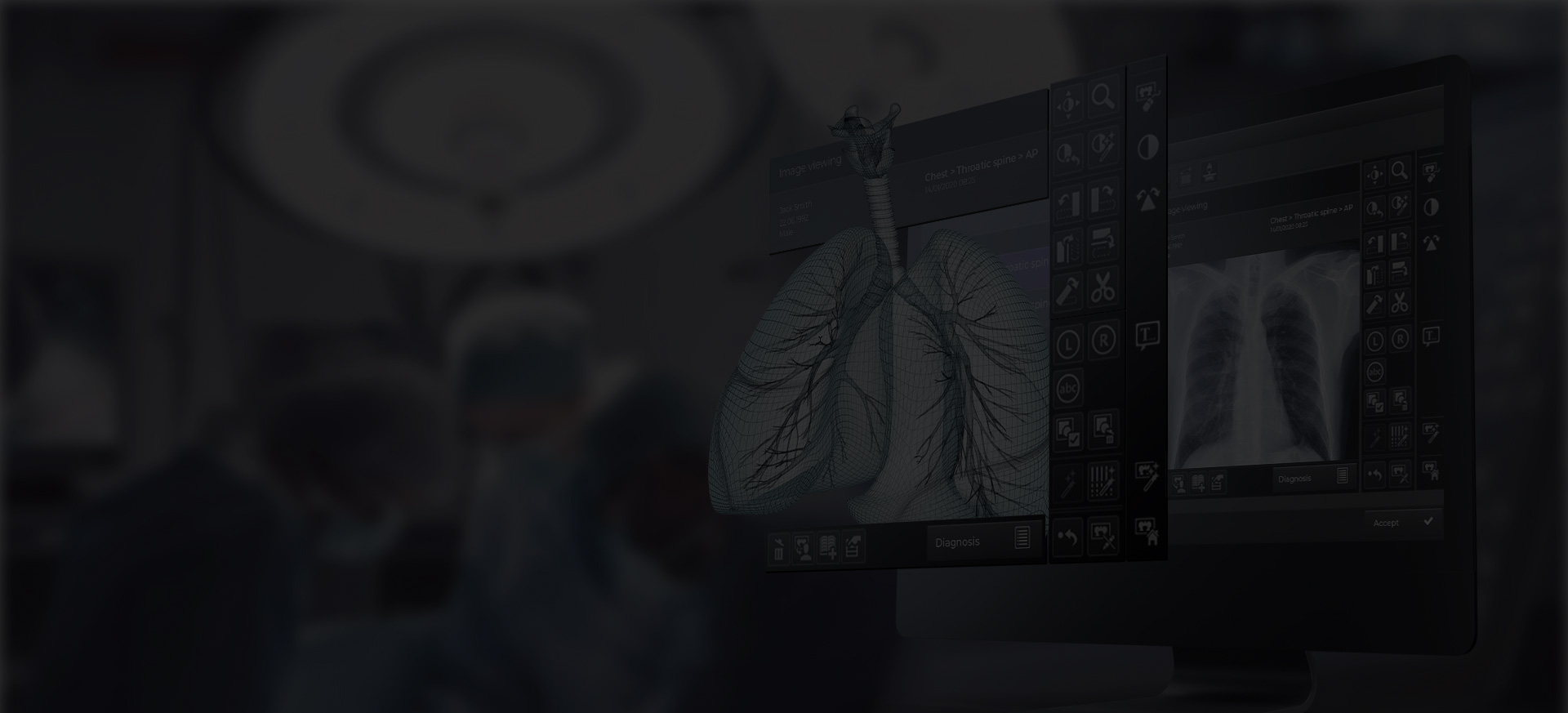
Detect anomalies such as tumors or fractures faster than with traditional methods. Beyond imaging, custom AI computer vision solutions can assist your facility with analysis and optimizing hospital resources. They also support early, personalized care, and improve overall healthcare efficiency and access.
Integrated AI systems combine telehealth, wearable and non-wearable data, and clinical records to predict disease progression, recommend optimal therapies, and minimize side effects. Tailor treatment plans using genetic, clinical, and lifestyle data, with precision medicine that accounts for each patient’s individuality.
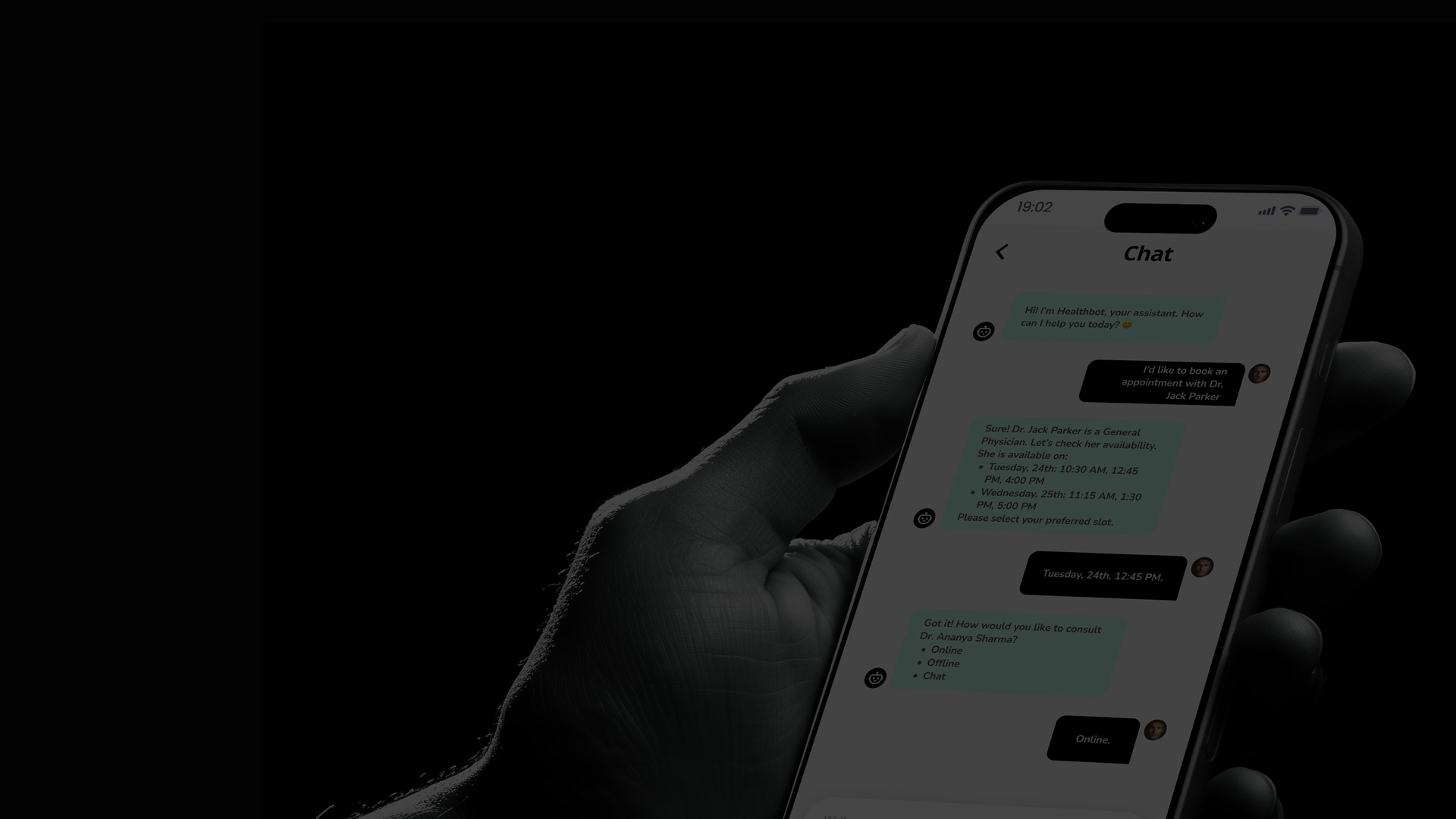
Employ virtual health assistants to deliver personalized guidance, medication reminders, and guidance for disease management. AI-powered chatbots and voice agents support administrative tasks, patient engagement, and triage. They also boost treatment adherence and enrich the patient’s experience.
Custom AI implementations improve resource allocation and handle administrative workflows such as scheduling, billing, and EHR management. Process document databases, corporate data, and clinical records to generate insights and improve revenue cycles.
We’ll help you explore the smartest ways to improve patient outcomes and expand access. Practical, measurable, and designed around your organization’s priorities.

Advanced AI models promise precision and efficiency in healthcare, but concerns like bias, opacity, and regulatory hurdles remain. Oxagile applies technical and ethical safeguards to deliver safe, explainable, and compliant AI deployment.

Data is secured with encryption, anonymization, and federated learning, allowing AI to learn safely across distributed datasets. All processes are ISO 27001 certified.

AI models are trained on representative datasets, with bias detection tools applied to identify and minimize disparities, improving equity across patient populations.

We prioritize model interpretability, helping clinicians access clear, auditable reasoning when possible to support trust and regulatory compliance.

Custom APIs, middleware, and interoperability frameworks connect AI solutions to existing EHRs and hospital IT systems without disrupting workflows.

Documentation and solution designs that align with industry regulations and support certification readiness.

Consent management, patient autonomy, fairness, and transparency are embedded throughout AI development and deployment, supporting responsible clinical use.
OpenAI GPT, GPT-5 • Anthropic Claude family • Google Gemini family • AWS Titan models • IBM Granite models
Meta Llama 3.x family • Mistral & Mixtral series • Qwen family • DeepSeek V-series & R-series • Microsoft Phi-3 family • Stability AI series
Long-context transformers (xLAMs) • Multimodal LLMs • Code-optimized models (e.g., Code Llama, StarCoder 2)
PyTorch • TensorFlow & Keras • scikit-learn • JAX • Hugging Face Transformers & Diffusers • PyTorch Lightning • JAX Flax • OpenAI & Anthropic toolchains • ONNX
LangChain • LlamaIndex • Nvidia NeMo • Vector Database • Sentence Transformers • Cohere Embed • Chunking, ranking, and hybrid search orchestration
Multi-agent orchestration • Tool-using & function-calling agents • Planning & reasoning support • Memory-augmented workflows • AutoGPT-style autonomous agents
Supervised, unsupervised, self-supervised • Contrastive • Clustering & metric learning • RL/RLHF • Few & zero-shot tuning • RAG & tool use • Multimodal & cross-modal
Choosing the right partner means finding an AI healthcare software development company with proven expertise in clinical workflows, regulatory compliance, and secure, scalable solutions. Such a partner delivers real-world impact in complex healthcare environments.

Recent advances in intelligent healthcare technologies enable predictive analytics, early disease detection, and precision medicine. By analyzing diverse datasets, from imaging to genomics, clinicians can make faster, more accurate decisions and provide highly personalized care.
Mobile and web applications connect seamlessly with EHRs, wearables, and IoT devices, helping clinicians make timely decisions and keeping patients actively engaged in their care. When paired with intelligent healthcare solutions, these tools support continuous, personalized treatment and better health outcomes.