
Patient intake, demographics, referral flows, insurance data, consent management, and longitudinal records spanning multiple systems and care settings.

Most organizations today need EHR-grade interoperability, even if what they’re running was built as an EMR. Electronic health records (EHR) share data across facilities and care networks, while electronic medical records (EMR) don’t. Our engineers work across a wide array of solutions and handle:

The difference between EMR and EHR isn’t just terminology. It determines the scope and the cost of what comes next. Let’s review your setup and give a clear answer.
 Hospital networksRegional clinicsMid-size hospitalsHealthcare ISVs
Hospital networksRegional clinicsMid-size hospitalsHealthcare ISVs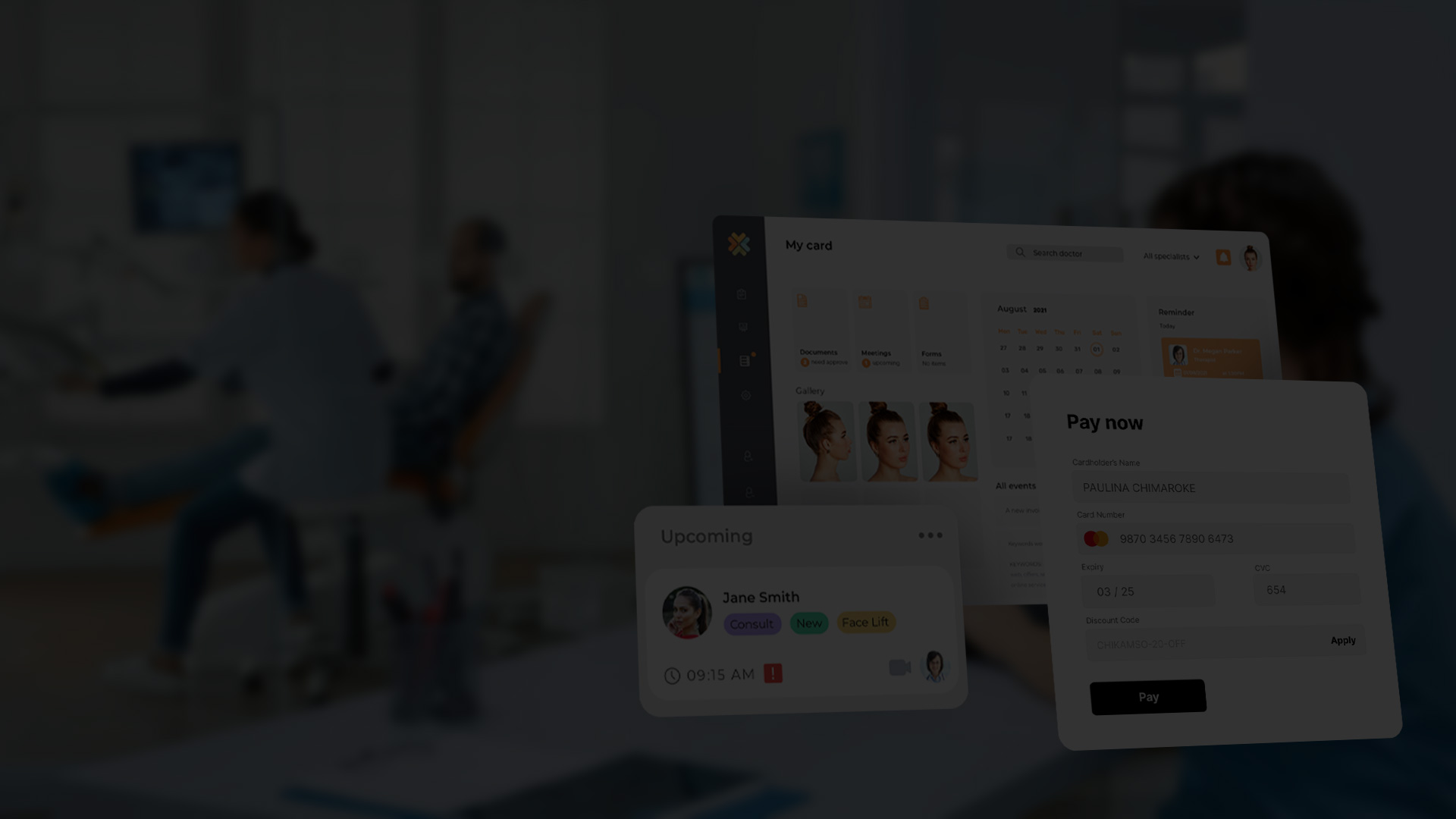




Most healthcare organizations aren’t starting from scratch, they’re running Epic, Oracle Health, or a legacy platform and need it connected to something else.
We build the integration layer: APIs, connectors, and middleware that bridge systems without touching the core platform.
HL7 FHIR is the current standard for clinical data exchange, and most organizations are either migrating toward it or are under regulatory pressure to comply.
We build the adapter layer that brings your existing systems into FHIR-compatible format without a full platform replacement.
When a hospital network needs to share patient data with regional partners, affiliated practices, or academic institutions, the infrastructure to do that reliably doesn’t exist out of the box.
We design and build the gateway layer that makes that exchange possible.
Moving clinical data between systems, or consolidating records from multiple sources, is where most EHR projects run into unexpected complexity.
We build migration pipelines, reconciliation workflows, and normalization layers that help healthcare teams synchronize records across fragmented environments.
When an off-the-shelf platform covers 80% of what you need but falls short on specific workflows.
We build the modules that fill the gap, without replacing the system your clinical staff already knows.
Before committing to an architecture, an integration approach, or a vendor, it helps to have engineers who’ve worked across these systems map out what the project involves.
That includes the implementation scope, compliance requirements, realistic timelines, and the main technical risks. We offer:
Healthcare infrastructure is rarely a single platform. Most organizations run a mix of EMRs, internal tools, partner systems, and legacy software, each holding a piece of the clinical picture.
 Records
Records Patient intake, demographics, referral flows, insurance data, consent management, and longitudinal records spanning multiple systems and care settings.
 Workflows
Workflows Provider-facing tooling for charting, care coordination, clinical documentation, and multi-department data exchange, built around how clinical staff work.
 Scheduling
Scheduling Appointment scheduling, provider calendars, billing integrations, claims processing, and revenue cycle workflows connected to the broader EHR environment.
 Diagnostics
Diagnostics Lab system integrations, diagnostic data pipelines, imaging metadata exchange, and synchronization between clinical and diagnostic environments.
 Portals
Portals Secure patient-facing applications for appointment management, records access, secure messaging, forms, and care journey interactions.
 Analytics
Analytics Clinical reporting pipelines, operational dashboards, interoperability reporting, and audit-ready data exports built on top of aggregated healthcare data.
The process we follow has been shaped by every engagement with healthcare providers. Stages below reflect decisions we’ve had to make on actual projects.

We map your infrastructure, like platforms, data flows, integration points, and establish what the project involves before any architecture decisions are made.

HIPAA, GDPR, HL7 FHIR, and TEFCA requirements are scoped at the start. We identify which standards apply and where compliance obligations sit in the timeline.

We define the integration layer: connector architecture, gateway design, data schemas, API contracts, FHIR compatibility, and authentication models.

Adapters, connectors, pipelines, custom modules, or migration logic, all built against your existing platforms without disrupting live clinical operations.

Integration testing, data integrity checks, security audits, and compliance validation run in parallel with development, not as a final gate.

Staged rollout with rollback capability and a structured handover. Full ownership of the codebase, data schema, and documentation stays with your team.

Most EHR projects get oversold at the discovery stage. We don’t propose platform replacements when the problem is a missing connector, and don’t quote FHIR compliance work before establishing whether it applies to your setup.
The scoping conversation comes first.

Connectors, gateways, FHIR adapters, and data migration pipelines are the core of what we do, not an add-on to a broader software development offer.
The engineers on your project have worked on data migration, security-grade integrations, and cross-system data flows across 20+ years of production software delivery.

Every engagement is structured so that the architecture, codebase, and data schema belong to you from day one.
No proprietary tooling that creates dependency, no lock-in through undocumented integrations. When the project closes, your team runs it independently.
HL7 FHIR R4 • HL7 v2/v3 • SMART on FHIR • IHE profiles • DICOM • REST & SOAP APIs • OAuth 2.0 / SAML
HIPAA Security & Privacy Rule • GDPR • TEFCA / ONC HTI-1 • HITECH • ISO/IEC 27001 • SOC 2 Type II readiness • OWASP ASVS secure coding • Audit logging & access control frameworks
Node.js • TypeScript • Python • Java / Kotlin • React / Next.js • React Native / Flutter • .NET (C#)
Microservices architecture • API-first architecture • Event-driven architecture • Serverless infrastructure • Monolithic modernization

Any developer that leads with a single figure is skipping the questions that actually determine cost: are you building net-new or integrating with an existing platform, which compliance frameworks apply (HIPAA, GDPR, TEFCA), and how complex is the data migration path.
A scoped integration project sits in a very different bracket than a full engagement. The right starting point is a scoping conversation, not a price list.
Ownership of the architecture, codebase, and data schema is established at the contract level before a line of code is written.
Proprietary frameworks and undocumented integrations are the two most common sources of lock-in any EHR or EMR software development company introduces. We use neither.
Every engagement is documented so your team can operate and extend the system independently when the project closes.
A production-grade, TEFCA-compliant EHR project is a multi-year commitment. TEFCA participation requires Common Agreement alignment, QHIN onboarding, and ongoing compliance obligations that don’t end at launch.
For most organizations, building FHIR-compliant integration layers on top of existing certified platforms is the more realistic path. If full certification is genuinely the requirement, we’ll scope it honestly, with timeline, engineering effort, and compliance workload included.